Interstage Site Care and Growth
Key Findings: Comparison of growth in Single-Ventricle infants followed for interstage care at surgical centers versus non-surgical centers
_________
Cardiology in the Young recently published a study online on January 2015: “Site of interstage outpatient care and growth after the Norwood operation”.
The NPC-QIC Research and Publication Committee has reviewed this article and a summary of the findings can be found below.
Main Finding from this Study:
Despite advances in surgical and medical care for infants with hypoplastic left heart syndrome after the Norwood procedure, the interstage period remains a time of high risk. One major problem these children suffer is poor growth, which has been the focus of recent efforts for improvement. Specifically, specific practices to improve growth include: use of home weight scales, monitoring for weight loss or for adequate weight gain, standard feeding evaluation in the hospital after the Norwood procedure, regular phone contact with cardiology clinicians, and dieticians at clinic visits.
This study was a retrospective comparison of two groups: infants who received their outpatient interstage care and cardiology visits at cardiac surgery centers that performed their Norwood procedure, and infants who received outpatient interstage care and cardiology visits at other cardiology sites. The authors of this study concluded that regardless of where infants received outpatient interstage care, their growth over the interstage period did not differ and remained below-average.
About this study:
Why is this study important?
As mentioned above, infants with hypoplastic left heart syndrome after the Norwood procedure are known to be at risk for poor growth, and our understanding of what specific practices are important to improve growth has advanced.Practices such as using home weight scales, maintaining regular phone contact with cardiology clinicians and dieticians, and monitoring for adequate weight gain are useful tools for families and cardiology care providers.However these practices require additional staff resources and equipment, and centers have been previously shown to vary in their use of these practices.
The authors of this paper hypothesized that infants who received outpatient interstage care at cardiac surgery centers would achieve better growth compared to infants who received care at other sites, since cardiac surgery centers are based in children’s hospitals with larger numbers of clinical staff.If either group of infants had poorer growth, then further measures (such as use of additional clinical staff or equipment) could be started to “close the gap” in growth.
How was this study performed?
This was a retrospective study of patients enrolled in the National Pediatric Cardiology Quality Improvement Collaborative single ventricle registry from 2008 to 2013. Infants who successfully completed the interstage period (from Norwood operation to stage 2 procedure) were included in the study, and infants were excluded if: the Stage 2 procedure was not completed due to cardiac transplantation or death before Stage 2, or if there was missing weight data.
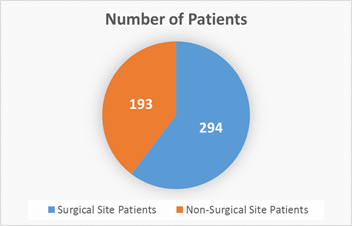
The infants were classified into two groups, based on data collected from the registry: the surgical site (SS) group, who had all interstage care given at the same center where the Norwood procedure was performed; and the non-surgical site (NSS) group, who had some or all interstage care given at another center distinct from the primary surgical center.
What were the results of the research?
487 infants total were analyzed: 294 infants in surgical site (SS) group, 193 infants in non-surgical site (NSS) group.
By Norwood hospital discharge, infants in both groups were similar except that the SS group were less likely to have hypoplastic left heart syndrome, and were slightly older at Norwood hospital discharge.
Specifically in terms of growth, infants in both groups had similar weight-for-age z-scores (a statistical measure for normal values of growth for a specific age).
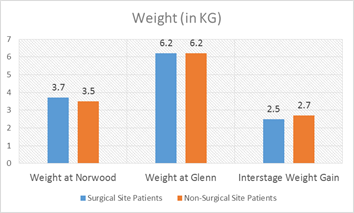
By the end of the interstage period, infants in both groups had similar weights (including similar weight-for-age z-scores). When looking at other measures of growth such as average weight gain per day, there were also no differences between the two groups.
When looking at all infants included in the study, the authors found that 29% were severely underweight (had very low weight-for-age z-scores) by stage 2 procedure.
Average daily weight gain during the interstage period was also not different between the two groups – 22.4 ± 6.4 g/day in the surgical site group versus 22.7 ± 6.3 g/day in the non-surgical site group (p =0.61).
What are the limitations of this study?
This was a retrospective study using data from a national database, and some patients (20% of infants enrolled) could not be included in the study due to inadequate or missing data. Although this study included patients from many cardiac centers in North America, it may not be representative of outcomes for patients at other centers.
The authors compared two groups of patients in this study: infants who had interstage care given only at the center where their surgery was performed, and those who had interstage care given at another site. Infants who had some care given at both sites were included in the non-surgical site group, but may have variable involvement of the surgery center team (including dieticians, etc.). The authors state these details were not defined further in the database (and thus could not be evaluated further), but were able to show no difference between groups in use of home weight scales or monitoring for interstage growth “red flags.”
What are the takeaway messages considering the results and limitations of this study?
For infants after the Norwood procedure, weight gain during the interstage period is not affected by the site of interstage outpatient care. However, a significant amount (nearly one-third) of infants studied were severely underweight by their stage 2 palliation surgery. Previous studies have demonstrated that specific practices, such as use of home weight scales and regular phone contact with cardiology clinicians/dieticians, are associated with improved weight gain in those infants who receive it. Current efforts through the NPC-QIC are underway to reduce variation and increase use of these practices.
Patel MD, Uzark K, Yu S, Donohue J, Pasquali SK, Schidlow D, Brown DW, Gelehrter S. Site of interstage outpatient care and growth after the Norwood operation. Cardiol Young. 2015 Jan 2:1-8.